 English page
English page Japanese page
Japanese page

 HOME
HOMEIntroduction of the department
New Department: Department of Cardiovascular and Thoracic Surgery
Clinical Professor of the Thoracic Surgery Group
Kichizo Kaga
 Upon the reorganization of surgical departments at Hokkaido University Medical School, our group will be a part of the newly established Department of Cardiovascular and Respiratory Surgery. The “Respiratory Surgery Group” is a former Second Surgery Group (Tumor Surgery Group) at Hokkaido University. As a part of the reorganization plan that establishes departments based on the different organs, the former Second Surgery Group became the “Second Surgery Group” of the Department of Digestive Surgery. Our Respiratory Surgery Group joined the Department of Cardiovascular Surgery to form the “Department of Cardiovascular and Respiratory Surgery”, which belongs to the field of thoracic surgery. We believe that this represents a new approach for the collaborative treatment system. We will introduce the history of our group and future vision from the view point of “Respiratory Surgery”, the name of the new treatment unit at Hokkaido University.
Upon the reorganization of surgical departments at Hokkaido University Medical School, our group will be a part of the newly established Department of Cardiovascular and Respiratory Surgery. The “Respiratory Surgery Group” is a former Second Surgery Group (Tumor Surgery Group) at Hokkaido University. As a part of the reorganization plan that establishes departments based on the different organs, the former Second Surgery Group became the “Second Surgery Group” of the Department of Digestive Surgery. Our Respiratory Surgery Group joined the Department of Cardiovascular Surgery to form the “Department of Cardiovascular and Respiratory Surgery”, which belongs to the field of thoracic surgery. We believe that this represents a new approach for the collaborative treatment system. We will introduce the history of our group and future vision from the view point of “Respiratory Surgery”, the name of the new treatment unit at Hokkaido University.
History of thoracic surgery
- Thoracic surgery in our country initially started out as “lung surgery” for the treatment of pulmonary tuberculosis (the first generation). During this era, segmentectomy was often performed to maintain lung function in the midst of benign disease. However, due to advances in chemical therapies, the incidence of pulmonary tuberculosis decreased and the main tasks for the department shifted to lobectomy for the treatment of lung cancer (the second generation). Extended surgery and combined resection were also performed during this period; however, results were inconsistent and therefore the application of extended operation was limited. At the same time, a new approach, Video-assisted Thoracoscopic Surgery (VATS), became available (the third generation). In the beginning, the procedure was not widely employed due to issues with safety and curability. However, it gradually became popular with the next generation of surgeons and is now used throughout the country. Although the procedure is still under development, it is becoming a standard approach in the area of respiratory surgery.
Thoracic surgery in Hokkaido
 click for magnifyerThe primary cause of cause-specific mortality in Japan is cancer, with lung cancer as the leader since 1995. Yearly mortality of males and females has reached 50,395 and 19,418, respectively (“Vital Statistics” 2010 by the Ministry of Health, Labor and Welfare) and the numbers are still rising. In Hokkaido, the mortality rate for lung cancer is 18.8 (mortality rate of the population younger than 75 years old per 100,000 people. The national average in 2009 was 14.9), which is the highest in Japan. This is largely due to the high smoking rate in males (35%) and females (16%; the highest in Japan). A low rate of medical examinations may be an additional cause. Thus, medical facilities are not solely to blame for the delayed response against cancer. An integrated approach from national and private organizations is needed.
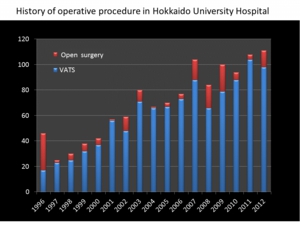
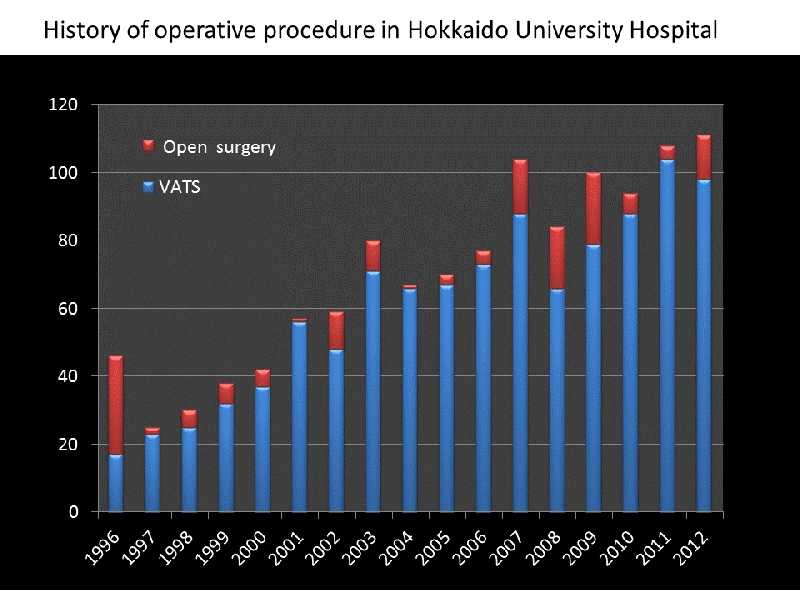
click for magnifyerThe primary cause of cause-specific mortality in Japan is cancer, with lung cancer as the leader since 1995. Yearly mortality of males and females has reached 50,395 and 19,418, respectively (“Vital Statistics” 2010 by the Ministry of Health, Labor and Welfare) and the numbers are still rising. In Hokkaido, the mortality rate for lung cancer is 18.8 (mortality rate of the population younger than 75 years old per 100,000 people. The national average in 2009 was 14.9), which is the highest in Japan. This is largely due to the high smoking rate in males (35%) and females (16%; the highest in Japan). A low rate of medical examinations may be an additional cause. Thus, medical facilities are not solely to blame for the delayed response against cancer. An integrated approach from national and private organizations is needed.- At Hokkaido University, we started implementing video-assisted thoracoscopic surgery from early on and we played a leading role in establishing minimally invasive surgery. We established two windows methods and one window and puncture method, and succeeded in performing surgery with the smallest incision in the world. At the same time, we are also aggressively performing extended operations against progressive lung cancer in addition to surgery as multidisciplinary therapy. Thus, our group has two main objectives with regard to treatment and research: “limited operation such as segmentectomy to preserve respiratory function and minimally invasive surgery using a thoracoscope for early stage lung cancer”; and “assurance of safety and improvement of the treatment results of surgical resection combined with chemotherapy and radiotherapy against progressive lung cancer. Figure 1 shows the history of surgical procedures for malignant lung tumor at our university. It is apparent that the number of subjects
 receiving surgical treatment for malignant lung cancer is increasing. Also, the high ratio of minimally invasive surgeries is a characteristic of our respiratory surgery group. The other special feature of our university that is distinct from other general hospitals and centers is the presence of a support system from various other departments in related fields. By pursuing minimally invasive surgery further, treatment options will be expanded for elderly patients, a growing demographic in the future, as well as patients with a low tolerance to surgery. In order to reduce the mortality of lung cancer, it is essential to carry out comprehensive treatment together with related departments and to establish research collaborations with basic medical science departments. We will further enhance our expertise in each group and are also looking forward to future developments of the new department via collaborations between Cardiovascular and Thoracic Surgery Groups.
receiving surgical treatment for malignant lung cancer is increasing. Also, the high ratio of minimally invasive surgeries is a characteristic of our respiratory surgery group. The other special feature of our university that is distinct from other general hospitals and centers is the presence of a support system from various other departments in related fields. By pursuing minimally invasive surgery further, treatment options will be expanded for elderly patients, a growing demographic in the future, as well as patients with a low tolerance to surgery. In order to reduce the mortality of lung cancer, it is essential to carry out comprehensive treatment together with related departments and to establish research collaborations with basic medical science departments. We will further enhance our expertise in each group and are also looking forward to future developments of the new department via collaborations between Cardiovascular and Thoracic Surgery Groups.
Collaboration between the Thoracic Surgery Group and Cardiovascular Surgery Group
 By clarifying clinical evidence of progressive lung cancer, we are able to realize the limitations of surgical treatment. Of course, clinical evidence is not fixed; we must accumulate it by ourselves. However, surgical treatment is useless against systemic disease. Sometimes, surgical treatment is not effective even for local disease. An example is T3-4 lung (chest wall and spinal infiltration, and large artery infiltration). However, our group is now capable of performing reconstructing surgery following combined resection, combined resection under an artificial cardiopulmonary circuit, and combined resection of the aortic wall using stent placement. On the other hand, minimally invasive cardiovascular surgery (MICS) is used for coronary artery bypass and cardiac valve replacement. The Respiratory Surgery Group at Hokkaido University has been implementing thoracoscopic surgery from an early stage and the technique is now well established. We are expecting the development of new MICS procedures through collaboration with the Cardiovascular Surgery Group. Hokkaido University Hospital was approved as a heart transplantation facility in July, 2010. We have held numerous simulation surgeries and seminars on heart transplantation and are expecting to perform the facility’s first heart transplantation at a moment’s notice. There are eight approved lung transplantation facilities in Japan. Our goal is to perform transplantation of all types of organs in Hokkaido and we believe that this is our responsibility. We are moving toward the next generation of cardiovascular-respiratory treatment.
By clarifying clinical evidence of progressive lung cancer, we are able to realize the limitations of surgical treatment. Of course, clinical evidence is not fixed; we must accumulate it by ourselves. However, surgical treatment is useless against systemic disease. Sometimes, surgical treatment is not effective even for local disease. An example is T3-4 lung (chest wall and spinal infiltration, and large artery infiltration). However, our group is now capable of performing reconstructing surgery following combined resection, combined resection under an artificial cardiopulmonary circuit, and combined resection of the aortic wall using stent placement. On the other hand, minimally invasive cardiovascular surgery (MICS) is used for coronary artery bypass and cardiac valve replacement. The Respiratory Surgery Group at Hokkaido University has been implementing thoracoscopic surgery from an early stage and the technique is now well established. We are expecting the development of new MICS procedures through collaboration with the Cardiovascular Surgery Group. Hokkaido University Hospital was approved as a heart transplantation facility in July, 2010. We have held numerous simulation surgeries and seminars on heart transplantation and are expecting to perform the facility’s first heart transplantation at a moment’s notice. There are eight approved lung transplantation facilities in Japan. Our goal is to perform transplantation of all types of organs in Hokkaido and we believe that this is our responsibility. We are moving toward the next generation of cardiovascular-respiratory treatment.
Final remarks
- the medical field in the future. For us, it is important not only to build an attractive future for surgery and guide young surgeons but also to make an effort to introduce the appeal of surgery. Please look forward to the new Department of Cardiovascular Respiratory Surgery.
(From the 2013 Hokkaido University School of Medicine Alumni Newsletter.)
![]()